The Culture Of MAID: How Assisted Death Became Normal In Canada
 By PNW Staff May 28, 2026
By PNW Staff May 28, 2026
Share this article:
The details surrounding the death of 45-year-old Ontario man Thomas Dillon are so shocking that many Canadians could be forgiven for thinking the story was satire.
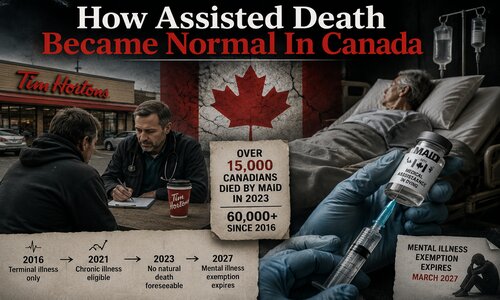
A doctor reportedly assessed Dillon for euthanasia outside a Tim Hortons coffee shop, exchanged personal text messages with him about ending his life, and later drove him to the location where he would receive a lethal injection. Yet this was not fiction. It was another real case within Canada's rapidly expanding MAID system -- Medical Assistance in Dying -- a program that has now become one of the fastest-growing causes of death in the country.
What is perhaps even more alarming than the circumstances themselves is the response. The physician involved, Dr. James MacLean, was not stripped of his ability to perform MAID. Instead, he agreed to six months of supervision and additional education after Ontario regulators concluded that his conduct exposed patients to potential harm.
For many Canadians watching this unfold, the story raises a haunting question: if this does not trigger serious consequences, what exactly are the safeguards?
According to reporting from the National Post and The Globe and Mail, Dillon suffered from Crohn's disease but also battled depression, social isolation, substance abuse, and previous suicidal ideation. He qualified under Canada's "Track 2" MAID category, meaning his natural death was not reasonably foreseeable.
That distinction matters enormously.
When Canada first legalized euthanasia in 2016, many supporters assured the public it would be limited to terminally ill patients already nearing death. But over time, the system expanded dramatically. First came eligibility for chronic illness and disability. Then came Track 2 approvals for those not dying but suffering physically or psychologically. Canada even prepared to extend MAID eligibility to those suffering solely from mental illness before temporarily pausing implementation amid growing backlash from psychiatrists, disability advocates, and lawmakers concerned about the lack of safeguards.
But that pause is not permanent.
Unless the law changes again, the current exemption preventing Canadians from accessing MAID solely for mental illness is set to expire in March 2027. That means individuals suffering from conditions such as severe depression, PTSD, bipolar disorder, schizophrenia, or other psychiatric illnesses could eventually qualify for state-assisted death even if they are physically healthy.
That reality has stunned critics both inside and outside Canada.
Psychiatrists in Canada and Europe have repeatedly warned that determining whether mental suffering is truly "irremediable" is deeply subjective. Mental illness often fluctuates. People who experience suicidal despair can later recover, stabilize, and regain purpose through treatment, community support, medication adjustments, counseling, or spiritual intervention. Critics argue that introducing euthanasia into mental-health treatment fundamentally changes the role of medicine itself -- from preventing suicide to facilitating it.
The Dillon case already illustrates how blurry those lines can become.
According to reports, Dillon's family believed his desire to die was tied heavily to untreated depression, isolation, addiction struggles, and emotional suffering. Yet there was reportedly little documented effort to involve family members in the assessment process despite their concerns. The physician's text exchanges allegedly included comments minimizing the family's objections. At one point, according to reports, the doctor wrote to Dillon: "You are the one ending your life and not them."
The line between compassionate medical care and active encouragement begins to blur dangerously when doctors move from detached assessors to emotional participants in the death process itself.
Even more troubling was another complaint involving the same physician. In that case, MacLean reportedly failed to administer one of the required drugs during a MAID procedure. After initially being pronounced dead, the patient reportedly began breathing again after the doctor had already left the home. He later returned and administered additional drugs.
Imagine if such failures occurred during any other serious medical procedure. The public outcry would be enormous.
Yet in Canada's MAID system, critics increasingly argue accountability appears remarkably limited.
Dr. Ramona Coelho, a former member of Ontario's MAID death review committee, warned that "important gaps in oversight and accountability remain." Her concerns echo a growing chorus of physicians, disability advocates, and mental-health professionals who fear Canada has moved far beyond protecting the terminally ill and into something far darker: a system where death can become the path of least resistance for vulnerable people struggling with suffering, poverty, isolation, addiction, disability, or depression.
According to Health Canada's latest MAID report, more than 15,000 Canadians died through MAID in 2023 alone -- roughly 1 in every 20 deaths nationwide. Since legalization, the total number has now surpassed 60,000 deaths.
Those numbers are staggering. What was introduced as a supposedly rare and tightly controlled exception has rapidly become normalized.
This is especially concerning given Canada's broader healthcare pressures. Wait times for specialists, mental-health treatment shortages, chronic pain support gaps, and overwhelmed healthcare systems continue frustrating patients nationwide. Critics increasingly fear some individuals may view MAID not because all options were exhausted -- but because support systems failed them first.
Over the past several years, controversial MAID stories have surfaced involving disabled veterans, individuals struggling with housing insecurity, and patients unable to access adequate medical care. Some Canadians now fear the country is slowly normalizing assisted death as a substitute for long-term compassion, treatment, and human support.
Supporters of MAID insist the system still includes safeguards and respects individual autonomy. But stories like Dillon's make it harder for many Canadians to believe the process remains as careful and restrained as originally promised.
A euthanasia assessment outside a coffee shop parking lot. A doctor personally driving a vulnerable patient to die. A failed lethal injection procedure. Minimal professional consequences afterward. And now a looming expansion that could soon make mental illness alone grounds for assisted death.
None of this sounds like a system operating with the gravity, caution, and scrutiny that ending a human life should demand.
A society does not fundamentally change overnight. It changes gradually -- one exception, one expansion, one normalization at a time.